Attention
If you click “Continue” below, you will leave the current site. TerSera is not responsible for the privacy policy of any third-party websites. We encourage you to read the privacy policy of every website you visit.
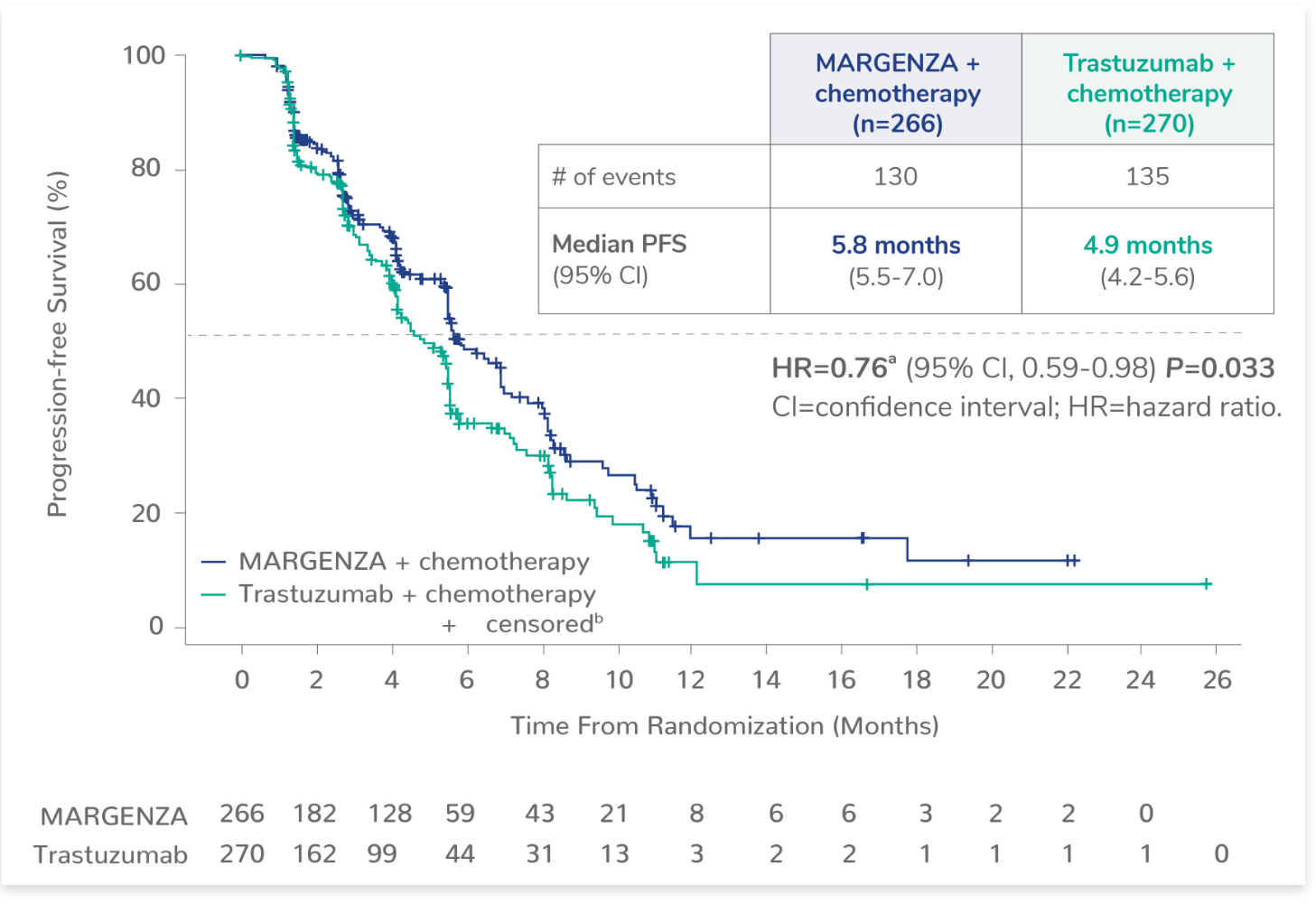
*PFS was evaluated by blinded independent central review (BICR).
aBased on stratified Cox Model.
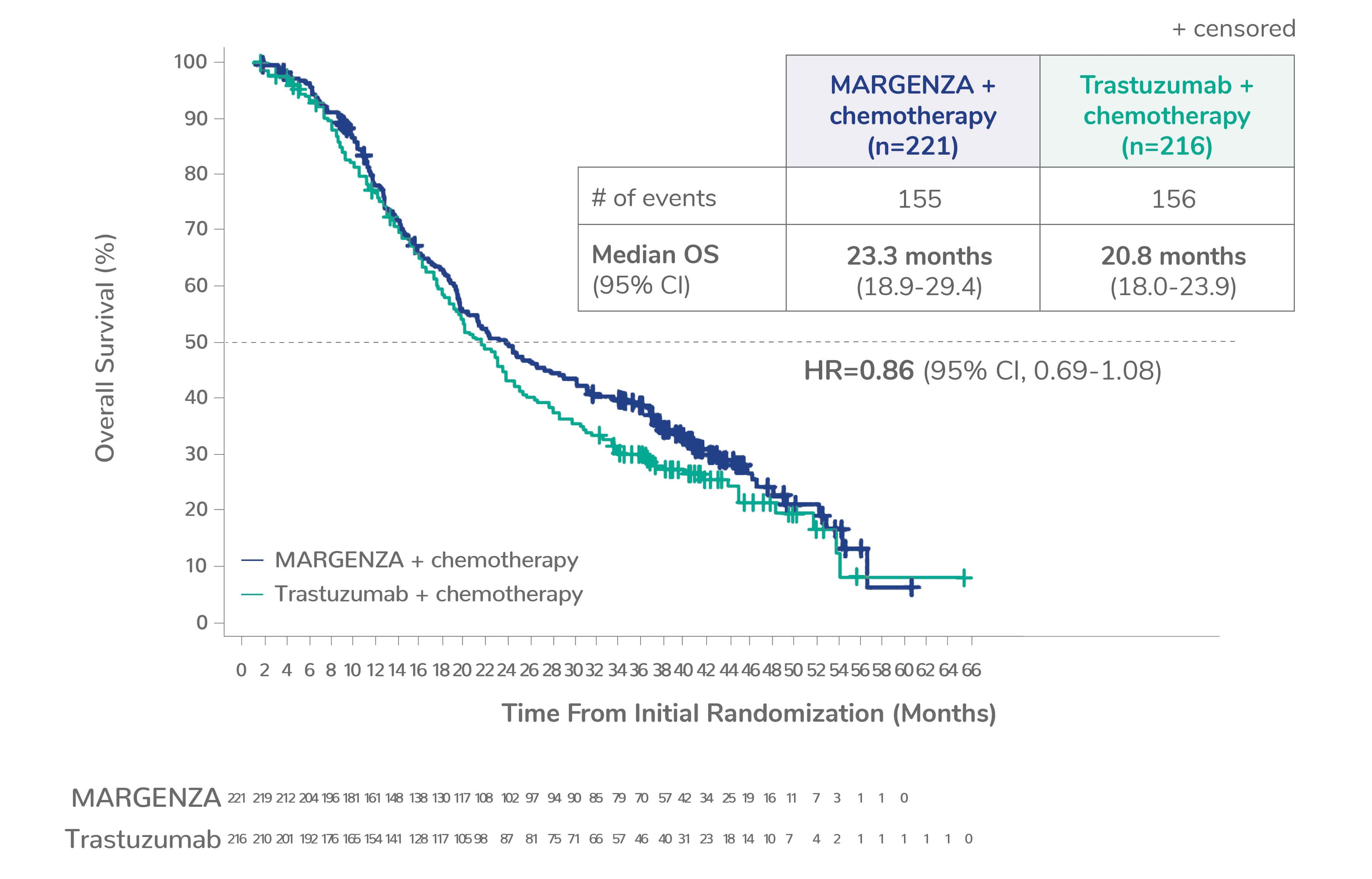
b+ censored indicates censored data.
Explore the SOPHIA Study, including Study Design, the complete list of Premedications, and Safety Profile seen in the study.
|
MARGENZA + chemotherapy |
Trastuzumab + chemotherapy |
|
|---|---|---|
|
OS2,c
Median (months) (95% CI) |
(n=266) 21.6 (18.9-25.1) |
(n=270) 21.9 (18.7-24.2) |
|
Objective response rate for patients with measurable disease1,d
Confirmed ORR (%) (95% CI) |
(n=262) 22 (17-27) |
(n=262) 16 (12-20) |
|
Duration of response1
Median (months) (95% CI)e |
(n=58) 6.1 (4.1-9.1) |
(n=42) 6.0 (4.0-6.9) |
cHR=0.95 (95% CI, 0.77-1.17). The OS analysis for the intent-to-treat population did not demonstrate a statistically significant advantage.
dAssessed per BICR.
eBased on Kaplan-Meier estimates.
See Exploratory PFS Analysis by CD16A Genotype
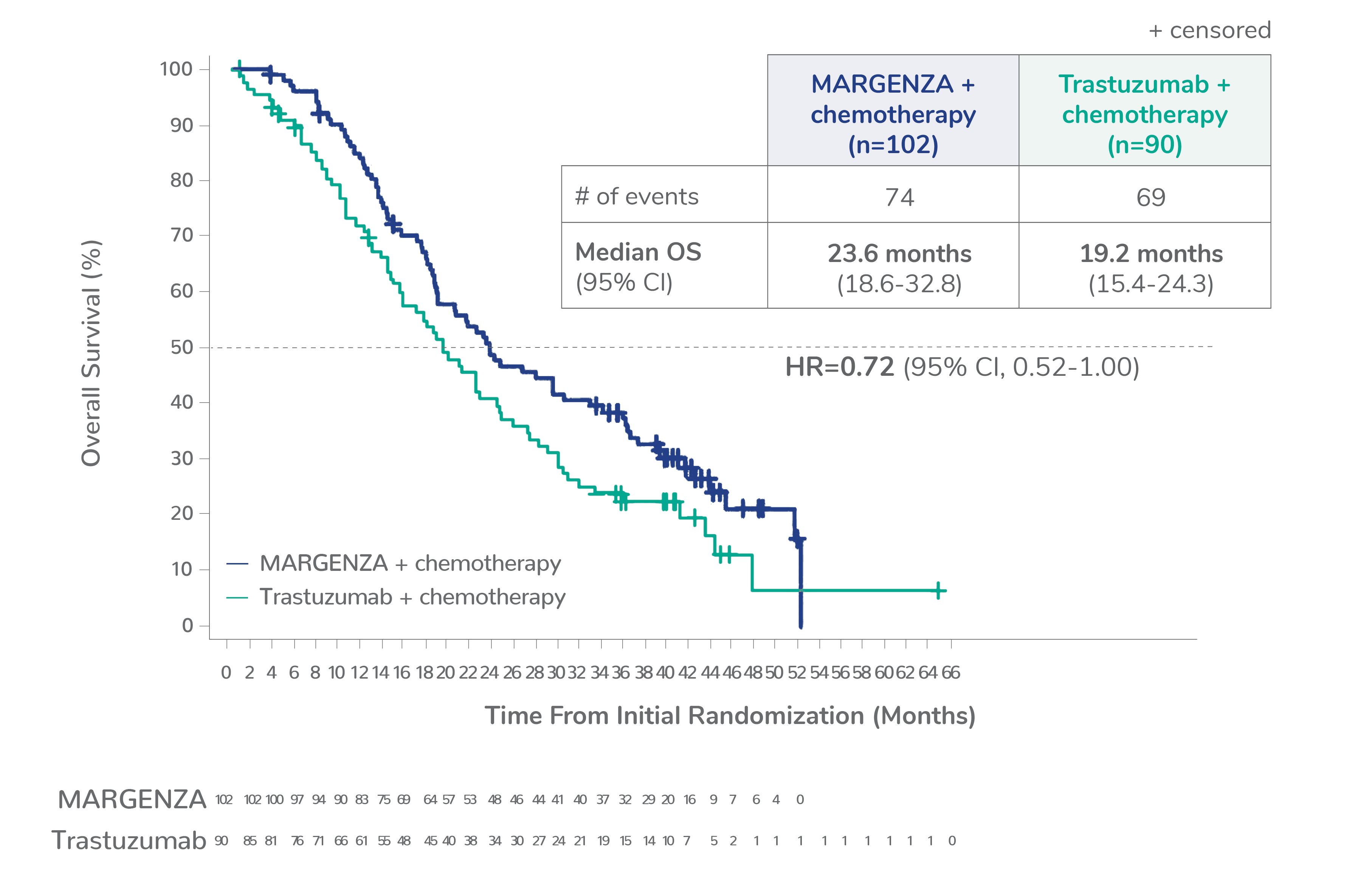
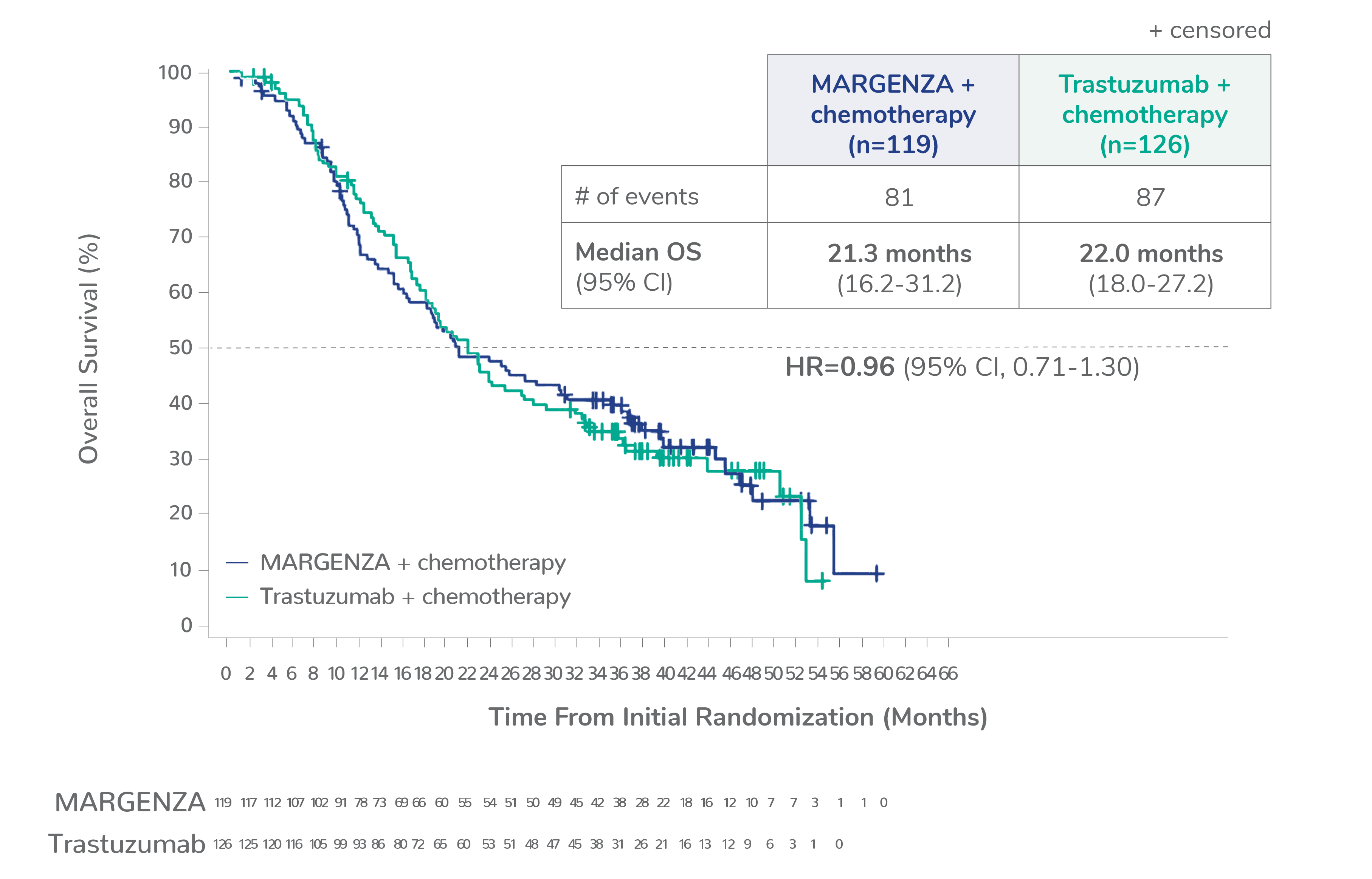
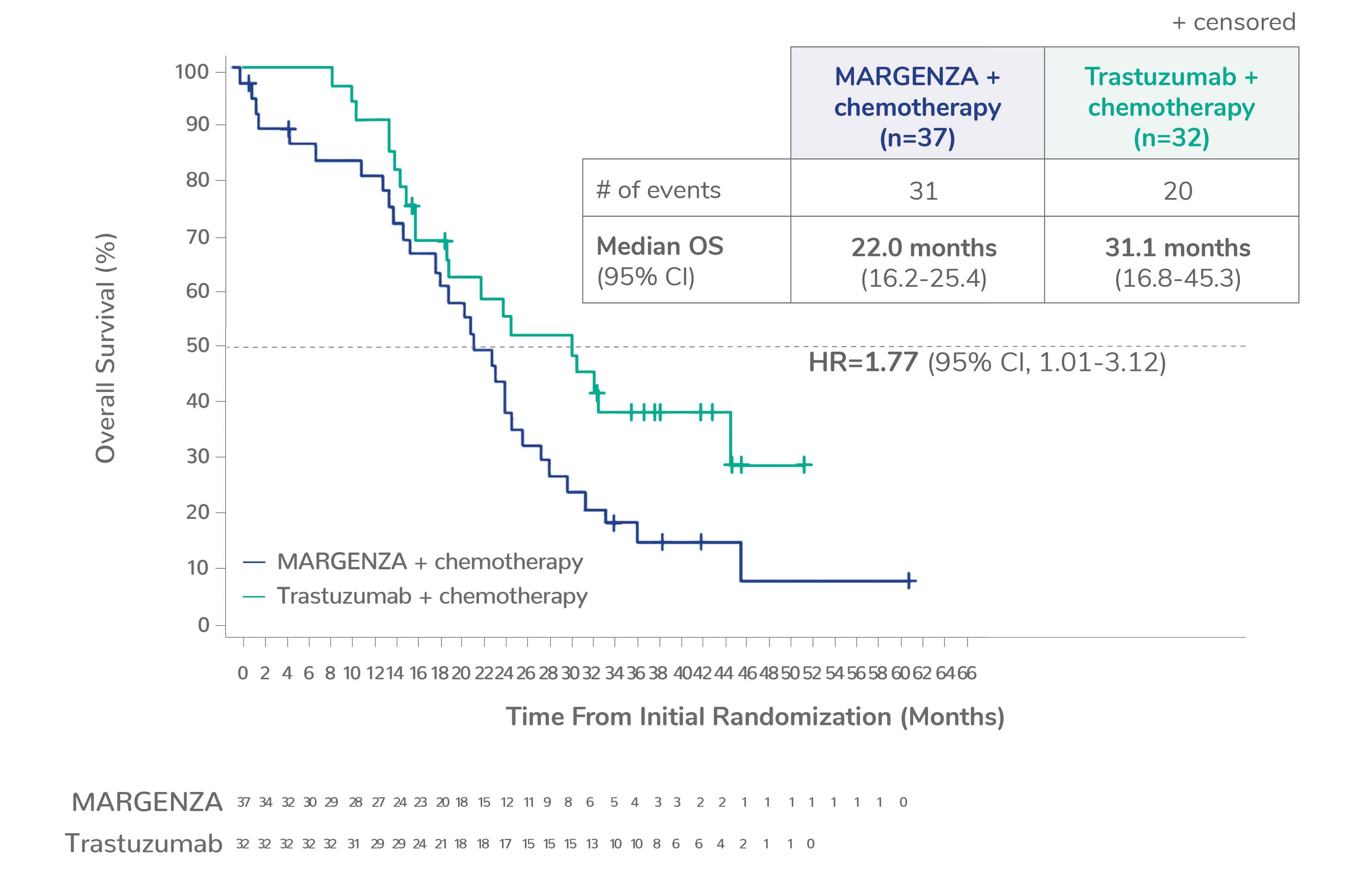
See Exploratory OS Analysis by CD16A Genotype
The efficacy and safety of MARGENZA plus chemotherapy compared with trastuzumab plus chemotherapy was evaluated in SOPHIA, a randomized, multicenter, open-label trial of 536 metastatic HER2-positive breast cancer patients† who have received two or more prior anti-HER2 regimens, at least one of which was for metastatic disease.
†IHC 3+ or ISH-amplified HER2‑positive.
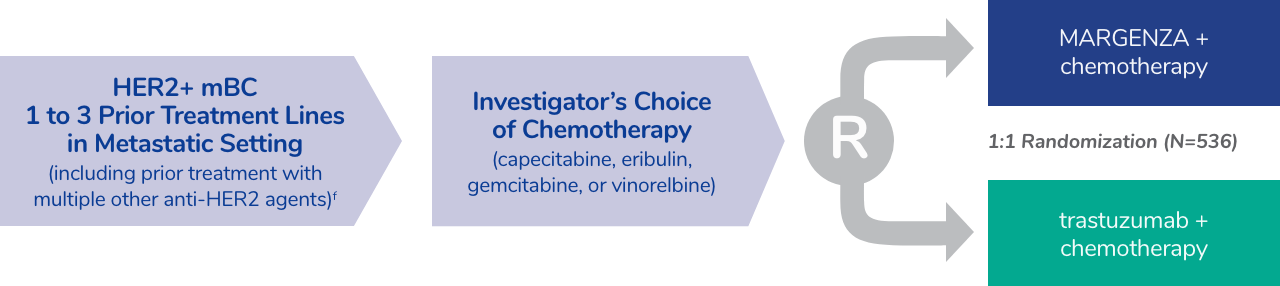
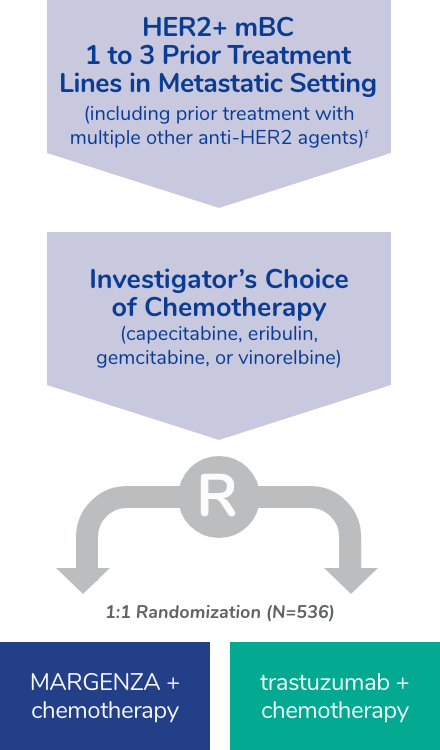
fThe median number of prior lines of therapy in the locally advanced/metastatic setting was 2 (range: 1-4). All study patients had previously received trastuzumab, all but 1 patient had previously received pertuzumab, and 91% had previously received ado-trastuzumab emtansine; 47% had visceral disease, 57% had bone metastases, 13% had brain metastases, and 60% were hormone receptor positive.
Premedications and prophylaxis for chemotherapy3
‡Effective April 1, 2020, the FDA requested manufacturers to withdraw all prescription and over-the-counter ranitidine drugs from market.
See dosage and administration information
Learn more about the
SOPHIA study
Safety of MARGENZA in combination with chemotherapy1
| Adverse Reaction | MARGENZA + chemotherapy (n=264) | Trastuzumab + chemotherapy (n=266) | ||
|---|---|---|---|---|
| All grades (%) | Grade 3 or 4 (%) | All grades (%) | Grade 3 or 4 (%) | |
| Fatigue/Asthenia | 57 | 7 | 47 | 4.5 |
| Nausea | 33 | 1.1 | 32 | 0.4 |
| Diarrhea | 25 | 2.3 | 25 | 2.3 |
| Vomiting | 21 | 0.8 | 14 | 1.5 |
| Constipation | 19 | 0.8 | 17 | 0.8 |
| Headacheg | 19 | 0 | 16 | 0 |
| Pyrexia | 19 | 0.4 | 14 | 0.4 |
| Alopecia | 18 | 0 | 15 | 0 |
| Abdominal painh | 17 | 1.5 | 21 | 1.5 |
| Peripheral neuropathyi | 16 | 1.1 | 15 | 2.3 |
| Arthralgia/Myalgia | 14 | 0.4 | 12 | 0.8 |
| Cough | 14 | 0.4 | 12 | 0 |
| Decreased appetite | 14 | 0.4 | 14 | 0.4 |
| Dyspnea | 13 | 1.1 | 11 | 2.3 |
| Infusion-related reaction | 13 | 1.5 | 3 | 0 |
| Palmar-plantar erythrodysesthesia | 13 | 0 | 15 | 3 |
| Extremity pain | 11 | 0.8 | 9 | 0 |
gIncludes headache and migraine.
hIncludes abdominal pain, abdominal discomfort, lower abdominal pain, and upper abdominal pain.
iIncludes peripheral neuropathy, peripheral sensory neuropathy, peripheral motor neuropathy, and neuropathy.
H1 antagonist=histamine H1 receptor antagonist; H2 antagonist=histamine H2 receptor antagonist; IHC=immunohistochemistry; ISH=in situ hybridization; IV=intravenous; OS=overall survival; PFS=progression-free survival.
1. MARGENZA® (margetuximab-cmkb). Prescribing Information. TerSera Therapeutics LLC.
2. Rugo HS, Im S, Cardoso F, et al. Phase 3 SOPHIA study of margetuximab + chemotherapy versus trastuzumab + chemotherapy in patients with HER2+ metastatic breast cancer after prior anti-HER2 therapies: Final overall survival analysis. Presented at San Antonio Breast Cancer Symposium on December 9, 2021 (#2484).
3. Data on File. Clinical Trial Protocol: CP MGAH22 04. Protocol Amendment 3.
Dosage and administration
information
CD16A-158F (FF or FV), n=437 (86%)
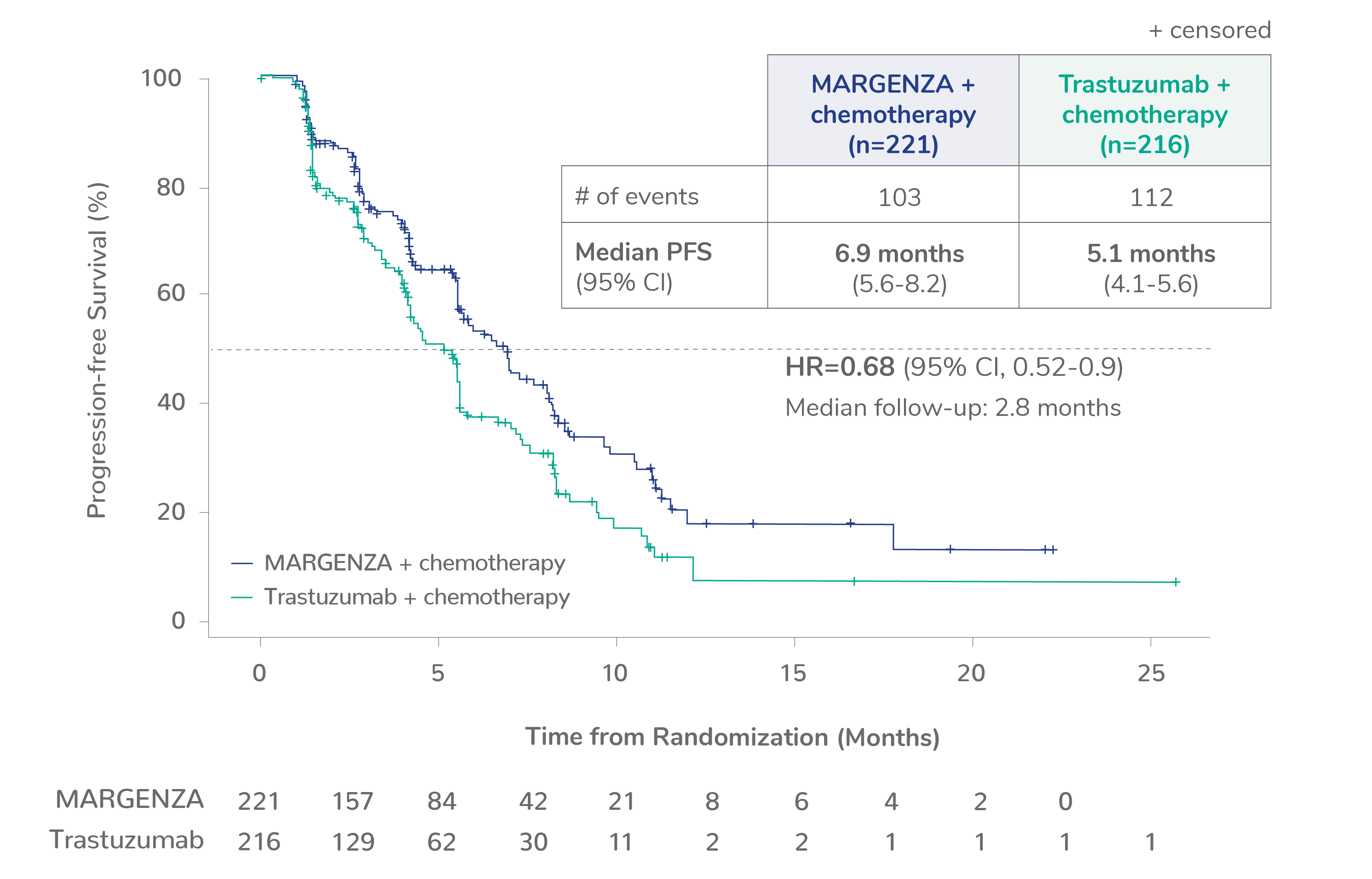
CD16A-158FF, n=192 (38%)
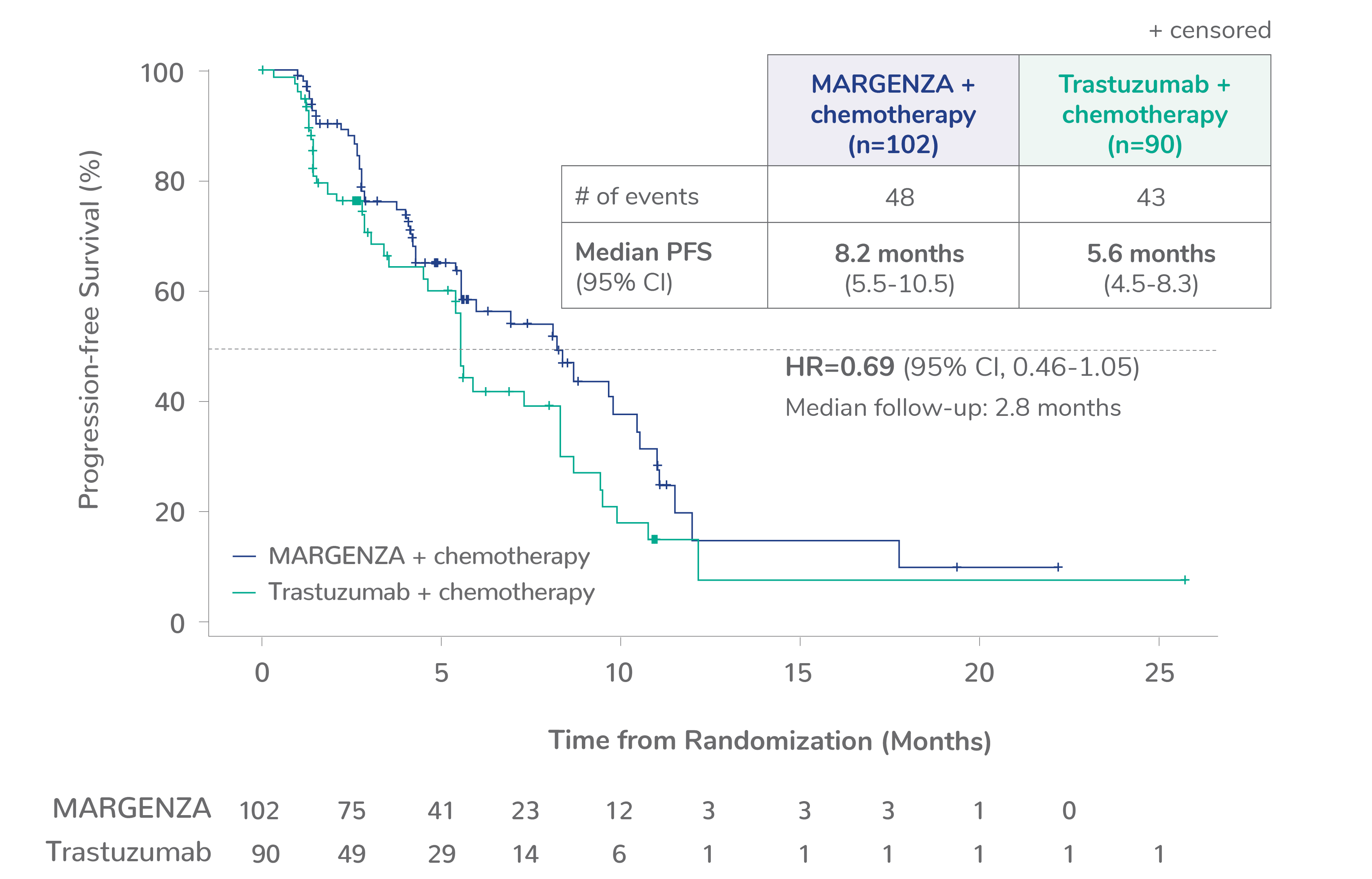
CD16A-158FV, n=245 (48%)
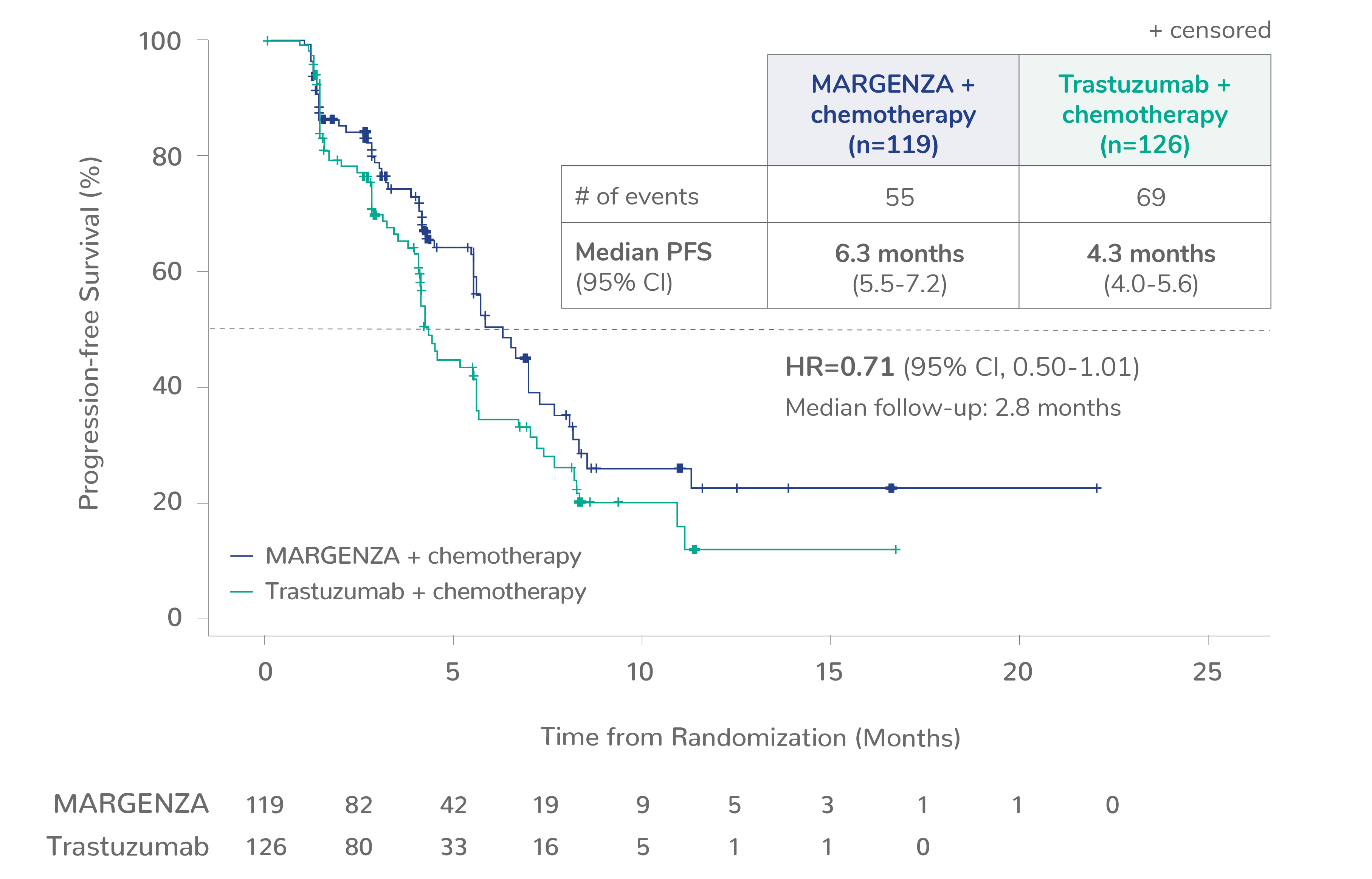
CD16A-158VV, n=69 (14%)
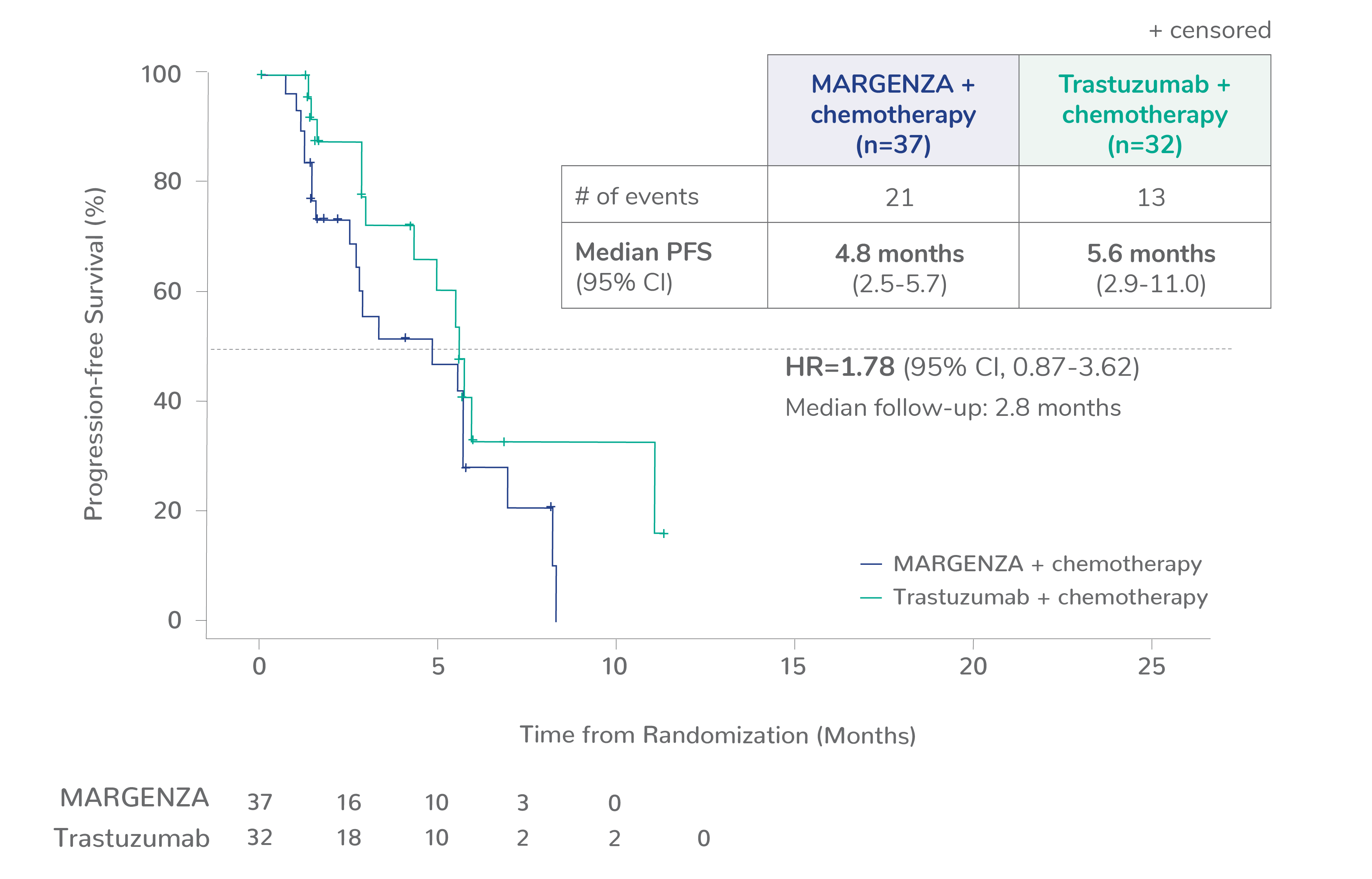
Limitation: These are exploratory analyses; therefore, the data require cautious interpretation and could represent chance findings.
a506 of 536 intention-to-treat patients were genotyped (94%).
CI=confidence interval; HR=hazard ratio.
1. Rugo HS, Im S, Cardoso F, et al. Efficacy of margetuximab vs trastuzumab in patients with pretreated ERBB2-positive advanced breast cancer: a phase 3 randomized clinical trial – Supplemental online content. JAMA Oncol. Published online January 22, 2021. doi: 10.1001/jamaoncol.2020.7932
CD16A-158F (FF or FV), n=437 (86%)
CD16A-158FF, n=192 (38%)
CD16A-158FV, n=245 (48%)
CD16A-158VV, n=69 (14%)
Limitation: These are exploratory analyses; therefore, the data require cautious interpretation and could represent chance findings.
a506 of 536 intention-to-treat patients were genotyped (94%).
CI=confidence interval; HR=hazard ratio.
1. Rugo HS, Im S, Cardoso F, et al. Phase 3 SOPHIA study of margetuximab + chemotherapy versus trastuzumab + chemotherapy in patients with HER2+ metastatic breast cancer after prior anti-HER2 therapies: Final overall survival analysis. Presented at San Antonio Breast Cancer Symposium on December 9, 2021 (#2484).
Important Information
If you click “Continue” below, you will leave the current site. TerSera is not responsible for the privacy policy of any third-party websites. We encourage you to read the privacy policy of every website you visit.
To find your NPI number, please fill out the information below.
Fields marked with an asterisk (*) are required.
The information contained in this section of the site is intended for US Healthcare Professionals only. Click Continue if you are a US Healthcare Professional.